Carpal tunnel syndrome
What is it?
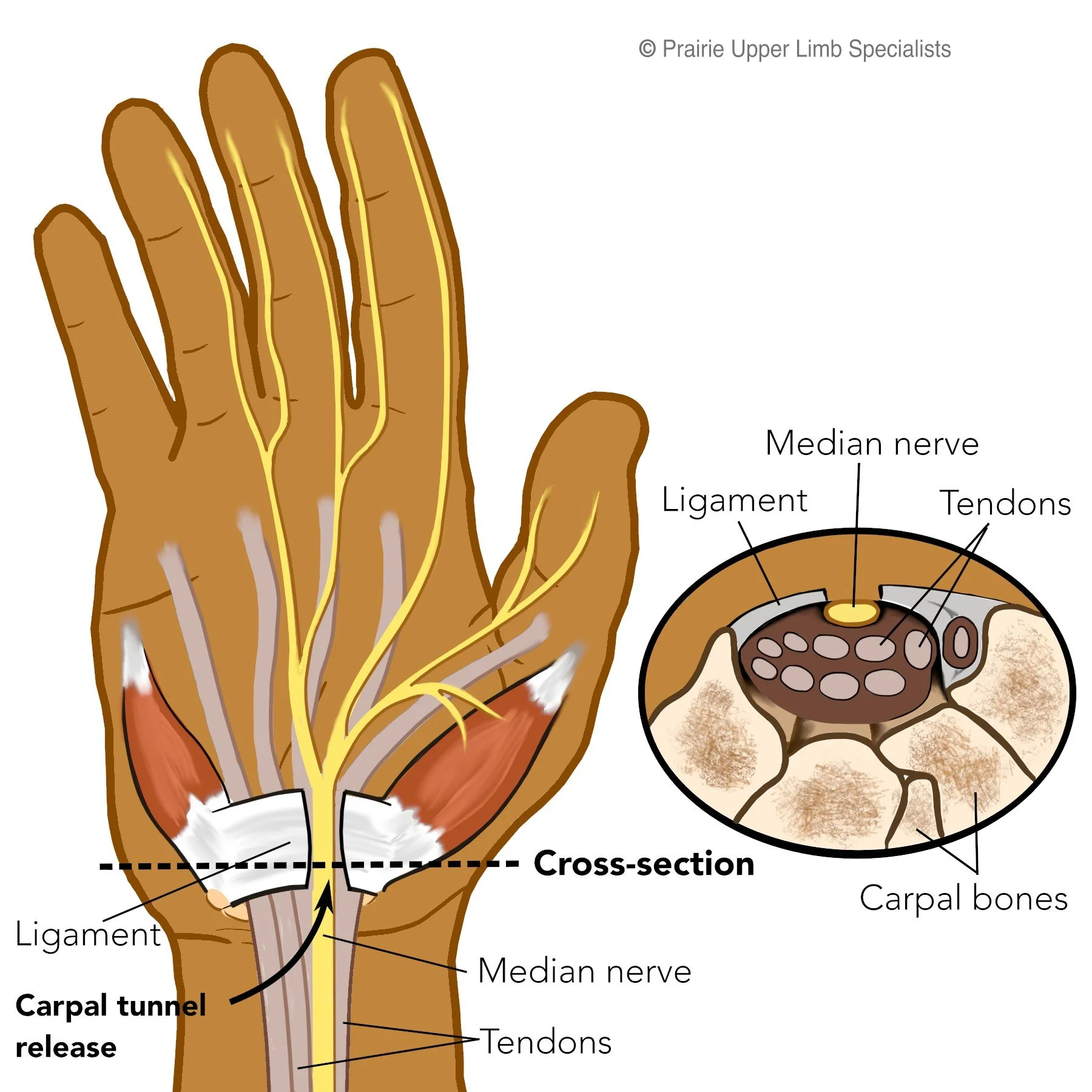
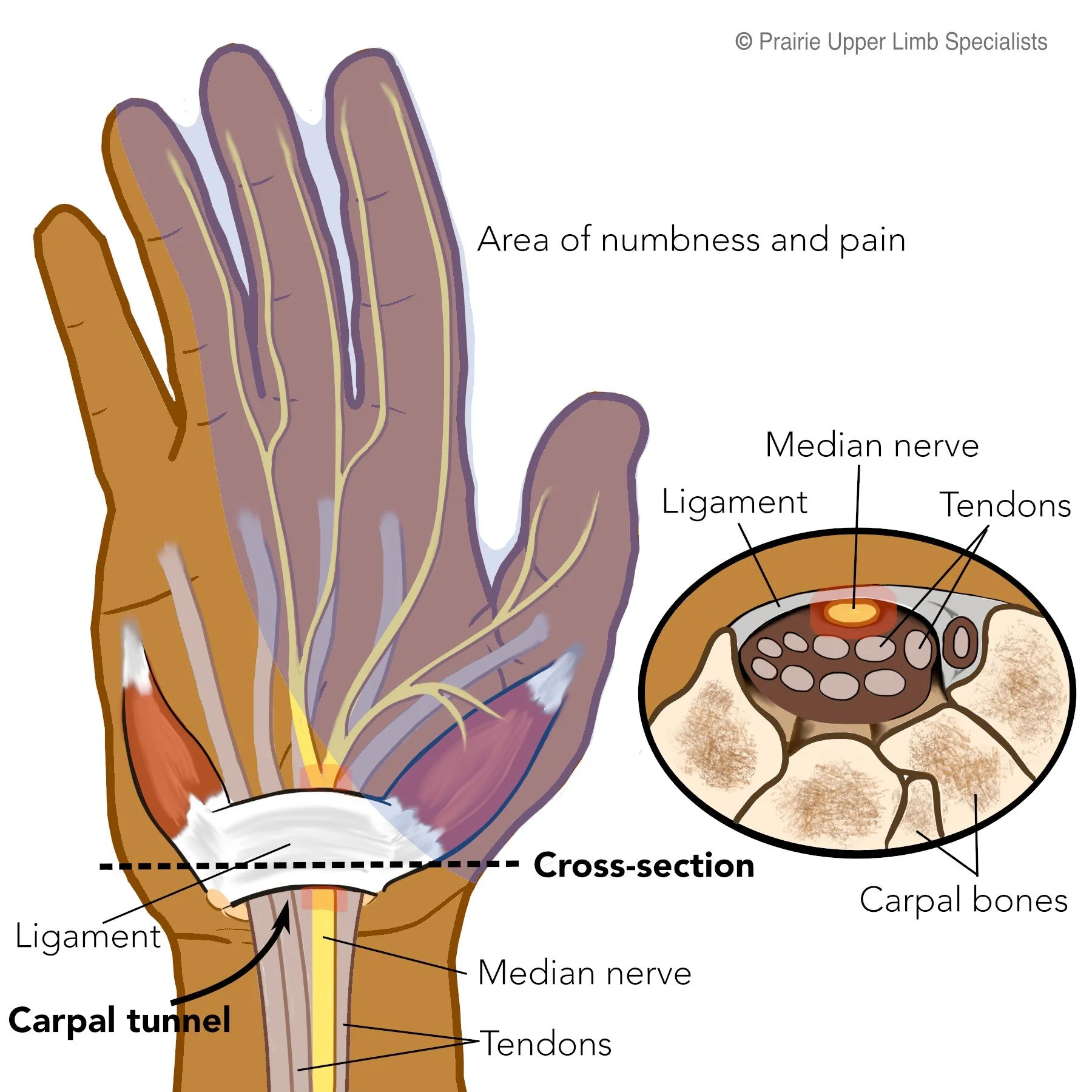
Carpal Tunnel Syndrome (CTS) is a condition of compression of the median nerve in the base of the hand.
What are the symptoms?
CTS most often presents with numbness and tingling in the thumb, index and middle fingers. It can also cause whole hand symptoms as well. Many people describe it as the hand “falling asleep.” It can present with shooting pains into the hand or the arm. It can be painful or non-painful. It is often worse with driving and at night. Although these are the common symptoms, it presents in many different ways.
What causes it?
There are 9 forearm tendons and the median nerve in the carpal tunnel at the base of the hand. If there is any swelling of the contents in the tunnel, it causes excessive pressure on the nerve. Swelling can be from tendinitis, repetitive trauma or arthritic swelling. It is common in pregnancy. Many times the cause is multifactorial (a combination of multiple factors). There is no evidence to link it to a specific occupation or activity. It is more common in patients in there 50s to 70s, but can affect any age.
How is it treated?
Generally the first treatment is without surgery. The most effective initial treatment is to wear a rigid wrist brace at night. This allows the nerve to heal overnight and often lessens the symptoms. Bracing will get rid of all symptoms for some people. Braces do not work for everyone and sometimes only lessens the symptoms. Cortisone injections are a very effective treatment. They are usually done with ultrasound to ensure the injection is placed right beside the nerve, but avoids nerve injury. It will cure some patients, but many have the symptoms come back months later. Nerve flossing with the guidance of a physiotherapist can also be helpful. There are many other treatments that may be successful as well, but are not as reliably successful as the treatments described above.
Description of Surgical Treatment
Surgical treatment is very successful but not guaranteed. Surgery involves dividing the tissue of the roof of the tunnel to relieve the compression. Although there are many different ways to perform it, our group performs a mini open procedure. It is a wide awake procedure with local anesthesia and no tourniquet. We perform it in the outpatient department of a hospital. There is a small amount of pain with the injection and no or minimal pain with the surgical release. It is very successful at relieving uncomfortable symptoms and pain at night. The palm will be sore for up to 3 months, with most returning to most activities by 6 weeks. A soft dressing is applied with no splint or cast.